INSUREDS ADDRESS No Street CITY STATE. The 1500 Health Insurance Claim Form 1500 Claim Form answers the needs of many health care payers.
Https Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf
You will recieve an email notification when the document has been completed by all parties.
Medical claim form 1500. Every medical claim is a legal document. INSUREDS NAME Last Name First Name Middle Initial 7. This document is locked as it has been sent for signing.
CMS 1500 Form also known as HCFA 1500 and has 33. Centers intended for Medicare health insurance and Medical preparing Services mainlined the Medical Claim Form 1500 the field of Medical Claim h billers MIBs is complete of business and authorities Plus as you hear regarding a deal to file the federal and state fees for totally free with 1040 variety variants H or perhaps curiosity less than 1 500. The advanced tools of the editor will guide you through the editable PDF template.
If you send a CMS 1500 claim form that you did not purchase but printed yourself it will be denied. Tips on how to fill out the Health claim form 1500 on the internet. NUMBER FOR PROGRAM IN ITEM 1 4.
To start the document utilize the Fill Sign Online button or tick the preview image of the blank. Also known as the Healthcare Financing Administration HCFA form the CMS-1500 form is used for claim reimbursement for several government insurance plans such as Medicaid Tricare and Medicare. CMS 1500 Field Location Required Field.
The HCFA 1500 claim form also known as CMS 1500 claim form as well. Enter your official contact and identification details. 49 rows CMS 1500 Form.
PATIENTS OR AUTHORIZED PERSONS SIGNATURE I authorize the release of any medical or other information necessary to process this claim. Other parties need to complete fields in the document. Download CMS Claim Form 1500 which is used by health care professionals to bill Medicare and Medicaid.
MEDICARE MEDICAID CHAMPUS CHAMPVA OTHER READ BACK OF FORM BEFORE COMPLETING SIGNING THIS FORM. ZIP CODE TELEPHONE Include Area Code 11. However the CMS pickup truck from the U.
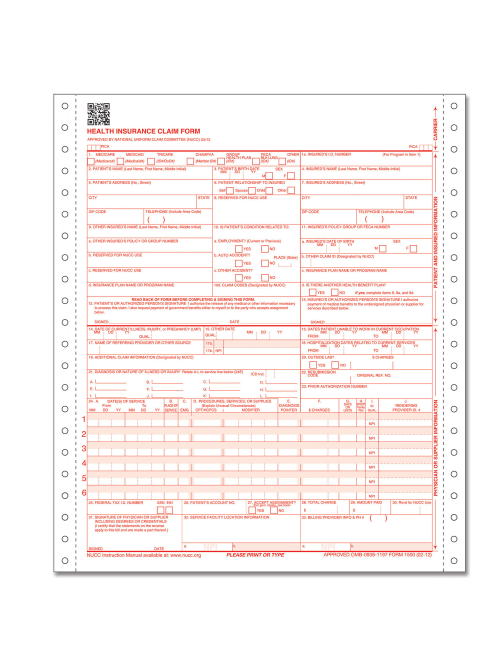
The CMS-1500 form is the standard paper claim form used by a non-institutional provider or supplier to bill Medicare carriers and Medicare administrative contractors MACs when a provider qualifies for a waiver from the Administrative Simplification Compliance Act ASCA requirement for electronic submission of claims. The CMS-1500 form is the standard paper claim form used by a non-institutional provider or supplier to bill Medicare carriers and Medicare administrative contractors MACs when a provider qualifies for a waiver from the Administrative Simplification Compliance Act ASCA requirement for electronic submission of claims. Health insurance claim form 1500.
The right-side margin of the CMS-1500 claim form has a note printed sideways that says carrier with arrows that indicate the top margin. HEALTH INSURANCE CLAIM FORM 1. The top half of the CMS-1500 medical claim form is used to report patient demographic and medical plan billing information.
The CMS 1500 Claim Form is the uniform or standard claim form used by a provider or supplier to bill Medicare and DMERCs durable medical equipment regional carriers when a provider qualifies for a waiver from the Administrative Simplification Compliance Act. Ad Search For Relevant Info Results. 1500 Health Inusrance Claim Form.
Get Results from multiple Engines. The CMS-1500 form popularly known as the Professional Paper Claim Form is a medical claim form that can be used by non-institutional providers and suppliers to bill claims. The form is used by Physicians and Allied Health Professionals to submit claims for medical services.
The Center of Medicaid and Medicare Services CMS form 1500 must be used to bill SFHP for medical services. You have successfully completed this document. Completed 2 July 2020.
Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical Services Provided Under the FEDERAL EMPLOYEES COMPENSATION ACT FECA the BLACK LUNG BENEFITS ACT BLBA and the ENERGY EMPLOYEES OCCUPATIONAL ILLNESS. This document has been signed by all parties. The carrier is the primary payor.
The CMS 1500 claim form uses a unique ink that allows the form to be scanned quickly and because of that the blank CMS 1500 form cannot be handwritten or printed by you. In addition to Medicare parts AB and for Medicare durable medical equipment Administrative Contractors. The CMS 1500 Claim Form is the uniform or standard claim form used by a provider or supplier to bill Medicare and DMERCs durable medical equipment regional carriers when a provider qualifies for a waiver from the Administrative Simplification Compliance Act ASCA requirement for electronic submission of claims.
A CMS 1500 with field descriptions and instructions is included in the link below. Claims must be made within 12 months after services are provided. Ad Search For Relevant Info Results.
Reset Form Print Form 1500 HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 0805. Get Results from multiple Engines. All items must be completed unless otherwise noted in these instructions.
It is the basic paper claim form prescribed by many payers for claims submitted by physicians other providers and suppliers and in some cases for ambulance services.